
Introduction of Astigmatism Contact Lens Practice:
- The astigmatic power that we get in retinoscopy or auto-refractometer is total astigmatism of our eyes.
- This total astigmatism can be of:
- Only corneal astigmatism.
- Corneal astigmatism and Internal Astigmatism together.
- Internal astigmatism (Residual Astigmatism) is the amount of astigmatism from crystalline lens (Lenticular Astigmatism) or other structures of the eye like vitreous, retina etc altogether or alone.
- Clinically, corneal astigmatism can be identified using a keratometer.
- But specifically, how much astigmatism is caused by lens or other internal structures of eye is not possible to identify.
- Thus, clinically we concerned about Corneal astigmatism & Internal Astigmatism which is important in Contact Lens fitting for astigmatic patient.
- Now, two questions arise:
- How to differentiate corneal & Internal astigmatism?
- Why does identifying internal astigmatism is important for CL fitting in astigmatic patient?
1. How to differentiate corneal & Internal astigmatism?
- The formula is:
TA = CA + IA
- Here,
- TA= Total Astigmatism.
- CA= Corneal Astigmatism.
- IA= Internal Astigmatism.
- If TA = CA + IA
IA = TA – CA
Example: A Patient with -1.0/-3.00 x 180 has keratometer reading of K1 42 @ 180 & K2 44D @ 90. What is the Total Astigmatism, Corneal Astigmatism & Internal Astigmatism?
.
.
.
.
- Here, total Astigmatism is -3.0D X 180 as we know that the astigmatism we get in retinoscopy or autorefractometer is total astigmatism.
- So Total Astigmatism is -3.0DC x 180.
Calculation of Corneal Astigmatism:
- The numerical difference between K1 and K2 is Corneal Astigmatism.
- CA = 44 -42 or CA = 2DC
- Here, Patient is having in horizontal (K1) 42D & in vertical (K2) 44D.
- Vertical meridian is 2D steeper which will require -2.0DC x 180 to correct.
- So, corneal astigmatism is -2.0 x 180.
Calculation of Internal Astigmatism:
IA = TA – CA
- Here,
- TA= -3.0DC
- CA= -2.0DC
- So, Internal Astigmatism will be:
- IA= -3.0 – (-2.0)
- IA= -3.0 + 2.0 or -1.0DC
So, Internal Astigmatism is -1.0DC x 180.
.
.
.
.
Why does identifying internal astigmatism is important for CL fitting in astigmatic patient?
- We know that hard contact lens (RGP) can correct up to 3DC of corneal astigmatism.
- So, if a patient has corneal astigmatism of up to 3DC, we can correct this astigmatism with a spherical hard contact lens without toric designs.
- Suppose a patient having a contact lens power of -1.0/-3.0 x 180.
- This can be corrected with a spherical -1.0D hard contact lens if the whole astigmatism is corneal.
- But if the patient has internal astigmatism of even 0.50DC a hard contact lens can’t correct it.
- Now, another question arises.
Why does Hard contact lens not able to correct even small amount internal astigmatism but can correct up to 3D corneal astigmatism?
To understand this, we have to understand how Hard Contact Lens corrects Corneal Astigmatism:
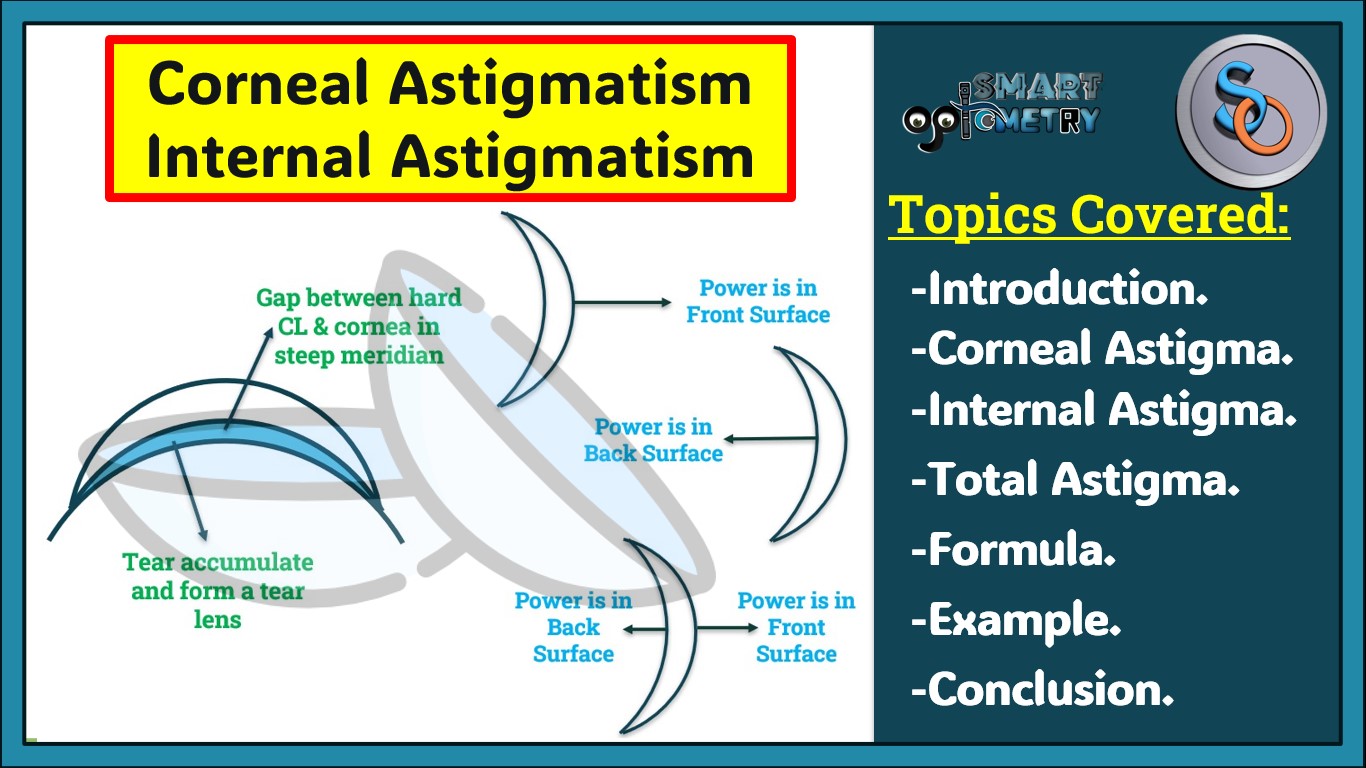
- We fit hard contact lens on flat meridian, so in the steeper meridian there will be gap between hard contact lens and cornea.
- In this gap/space tear accumulate and form a tear lens which can correct certain amount of corneal astigmatism (up to 3DC for Hard contact lens).
- Due to corneal astigmatism the curvature of meridians of cornea changes which allow tear lens to form when a spherical hard contact lens is fitted and correct certain amount of corneal astigmatism.
- But internal astigmatism occurred due to changes in the curvature of crystalline lens or other internal structures that doesn’t affect corneal curvature.
- Thus, tear lens can’t form in internal astigmatism and can’t correct any amount of internal astigmatism.
That’s why identifying type of astigmatism before prescribing a Toric or Spherical Hard Contact Lens its important to identify the type of astigmatism patient has.
.
.
.
.
- When a patient is having astigmatism, we identify whether patient is having corneal or Internal astigmatism.
- Then if corneal astigmatism is up to 3DC then go for a hard spherical trial lens.
- If a patient is having internal or corneal astigmatism of more than 3DC, then we have to choose a hard toric trial Contact Lens.
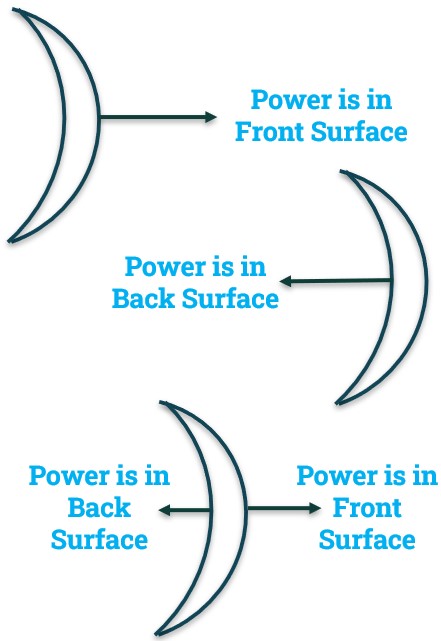
- If the patient is having internal astigmatism the front toric design is preferable as astigmatic power is incorporated in front surface of the Contact Lens that interact with eyelid not with the cornea.
- In back toric Contact Lens power is incorporated inner surface of the contact lens that can alter corneal shape if corneal astigmatism is not there.
- If both corneal & lenticular astigmatism is there then Bi-toric CL is also a choice.
- In Bi-toric contact lens, corneal astigmatic power is incorporated in back surface and internal astigmatic power is incorporated in the front surface of the lens.
Questions for You:
- Q-1: A patient with -1.50/-3.50 x 180, keratometer findings are K1 44 & K2 45. This patient has …………..?
- A. Corneal Astigmatism.
- B. Internal Astigmatism.
- C. No Astigmatism.
- D. Both A & B.
Type your Answer in Comment
.
.
- Q-1: A patient with -1.00/-2.00 x 180, keratometer findings are K1 44 & K2 44. Which toric design is ideal for this patient?
- A. Front Toric.
- B. Back Toric.
- C. Bi-Toric.
- D. None of these.
Type your Answer in Comment
- Check Our Courses: Ophthalmic Instrumentation, Clinical Refraction, Contact Lens, Binocular Vision, Dispensing Optics, MCQs in Optometry
- Download our App “Optometry Notes & MCQs” from Google Play Store.

2 Comments
You are right.
Stay with us for more Blog like this.
1. Ans- both a and b
2. Ans- Front toric